In America, we seem operate to under two modes – complacency or crisis. Not much in between. Everything’s OK until it’s not. Then we convene after the fact commissions to point fingers and prevent the same problem we missed. Remember the Rogers Commission to analyze the Challenger accident? The 9/11 Commission? Is the COVID-19 Commission next?
With the COVID-19 pandemic in the background, we see the juxtaposition of Spring Break revelers on Florida beaches contrasted with geographic hot spots in full quarantine.
First, a sincere voice of appreciation to our brothers and sisters providing healthcare around the world. They are working tirelessly to deliver care, prepare for the worst, and stay true to the Hippocratic oath. Also, a profound thanks to those in non-clinical fields, researching paths to treatment and prevention. Everyone has a role to play.
I’m of two minds on the coronavirus.
The realistic mortality rate is about 0.6%. It could be higher or it could be lower. Nobody really knows right now. The worst mortality rate for any influenza in our lifetimes was about 0.2%. And that horrible year was not a pandemic flu. The combination of COVID-19’s mortality rate plus its pandemic status makes me less sanguine than my typically sunny disposition allows.
That said, Taiwan and Korea have been crushing its spread. And if we had robust testing, we might see that the true mortality rate is far lower than reported.
The biggest benefit is the wake-up call for coming up with game plan for a really bad pandemic down the road. We got caught with our pants down. Avian flu, for example, has a mortality rate of 60%, though human to human transmission is extremely low. From the virus’ teleological perspective, you don’t want to kill the horse you came riding on.
The combination of a hypothetical high mortality rate and severe human to human transmission would put pressure on civil society. So, this wake-up call should get us ready for the next one.
On the plus side, the time period from identification of the virus, to genomic sequencing, to vaccine testing and therapeutic candidates has been nothing short of a miracle. There are bona fide therapeutic trials going on with existing compounds as I write. Early reports are showing positive results – faster recovery and fewer days of virus shedding. Plus, if you can spare $10k, you can order an onsite PCR machine from Biomeme and test all your neighbors.
Now for some perspective.
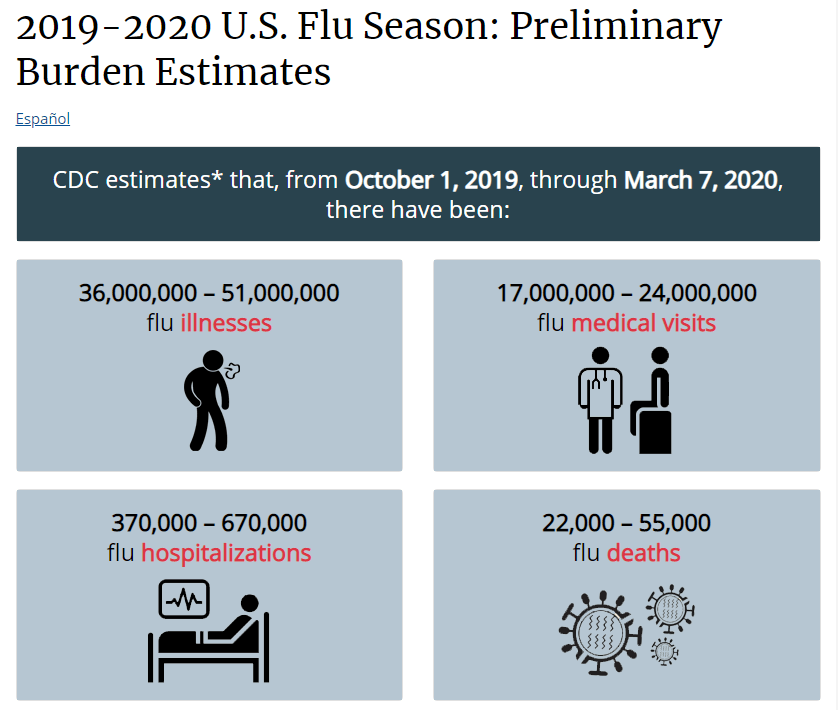
CDC reports that our current seasonal influenza is no walk in the park.
Still, we have vaccines and therapeutics for seasonal influenzas. Perhaps, that is why we do not panic over the seasonal flu.
Hopefully, once we have vaccines and therapeutics for coronavirus, the panic will subside.
In a community in which I participate, here is the back and forth dialogue:
“It is all on us and we can get through this by supporting our communities and helping to distribute accurate information.” – Dr. David Bray
“Imagine if we can make our response to this crisis our finest hour!” – Dr. Daniel Kraft
“Today the world is united against a common foe. We need to show up and do our bit.” – Nell Watson
“This is a chance as a civilization that we can mature, as a species, we can come together.” – Raymond McCauley
There’s a reasonable chance the curve will bend and we’ll all get back to business soon. Fingers crossed. Let us know your thoughts below.
Medical Justice helps great doctors practice great care with peace of mind. In the event you are thrust into a thorny medico-legal dilemma, we encourage our member physicians to call our STAT Medico-Legal HOTLINE (1-877-633-5878). This service is designed to deliver remedies to medico-legal obstacles ASAP. Our experts will walk with you until your obstacle is resolved.
If you are not a member of Medical Justice, we offer consultations to doctors in need of guidance.
Use the tools below to get in touch – or discover the benefits of membership. In addition to providing protection against medico-legal threats, we help doctors market themselves with patient reviews, powered by our eMerit platform. When combined, these services protect what is essential to the practice of good medicine – and they do away with what is detrimental.
About the Author
Jeffrey Segal, MD, JD
Chief Executive Officer and Founder
Dr. Jeffrey Segal, Chief Executive Officer and Founder of Medical Justice, is a board-certified neurosurgeon. Dr. Segal is a Fellow of the American College of Surgeons; the American College of Legal Medicine; and the American Association of Neurological Surgeons. He is also a member of the North American Spine Society. In the process of conceiving, funding, developing, and growing Medical Justice, Dr. Segal has established himself as one of the country’s leading authorities on medical malpractice issues, counterclaims, and internet-based assaults on reputation.
Dr. Segal was a practicing neurosurgeon for approximately ten years, during which time he also played an active role as a participant on various state-sanctioned medical review panels designed to decrease the incidence of meritless medical malpractice cases.
Dr. Segal holds a M.D. from Baylor College of Medicine, where he also completed a neurosurgical residency. Dr. Segal served as a Spinal Surgery Fellow at The University of South Florida Medical School. He is a member of Phi Beta Kappa as well as the AOA Medical Honor Society. Dr. Segal received his B.A. from the University of Texas and graduated with a J.D. from Concord Law School with highest honors.
In 2000, he co-founded and served as CEO of DarPharma, Inc, a biotechnology company in Chapel Hill, NC, focused on the discovery and development of first-of-class pharmaceuticals for neuropsychiatric disorders.
Dr. Segal is also a partner at Byrd Adatto, a national business and health care law firm. With decades of combined experience in serving doctors, dentists, and other providers, Byrd Adatto has a national pedigree to address most legal issues that arise in the business and practice of medicine.
Perfect Patient Dismissal & Termination Letters
Respond Masterfully to Negative Patient Reviews
Discover the Regulatory Landmines Most Doctors Miss





Here is a quick back-of-the-envelope calculation. If the US population is 327 million people and it cost $1,000 per Covid-19 test, that would be $327 billion dollars. And the pandemic would be able to be squelched in a matter of several weeks because we would know exactly who is infected and isolate them or treat them until the disease ran its course. The economy would go forward and the uninfected could go on with their lives. And $320 billion is much less that the rescue bills that Congress is proposing which may exceed $1 trillion. Yet, of course, it doesn’t cost $1,000 per test, and we wouldn’t have to test every man, woman, and child. South Korea, whose example is wonderfully relevant as they had their first episode on the same days as ours, January 19th, is way ahead of us on testing and public health spending. And their case numbers are receding already. They had learned from the pandemics of SARS (2003) and MERS (2015) while we were seemingly unlearning those lessons. Covid-19 should be a lesson for the importance of public health measures for our future.
“… if we had robust testing, we might see that the true mortality rate is far lower than reported.”
YES!!! We have a numerator, but so far, no denominator to tell us much about the bug. I’ve said that since the beginning and usually get blank stares.
On a related topic, do we know how the bug kills? We know that it causes a pneumonia. Is the purely viral pneumonia the cause of death? Or do they tend to be superinfections? In which case, making sure your pneumonia immunization would be potentially lifesaving.
Why is the bug worse in Italy, say, than here or even in Asia? Several possible explanations come to mind: 1) it’s a different, more virulent strain. maybe, unlikely, but maybe; 2) they have an older population and it affects the elderly disproportionately. Well, yeah, but why? 3) The smoke like chimneys over there. Has anyone looked at stratifying deaths by whether patients are (were) smokers, and their pack-year histories? If so, I haven’t heard about that parameter. A lot fewer Americans. smoke than do Europeans and Asians, and we seem to have a lot lower death rate than Italy does. Heck–so does China, at least as reported.
I have no idea how prevalent getting pneumonia vaccinations are in Europe.
There is an argument about testing. We are a huge country and it is much more difficult to get universal testing, especially when we have just HEARD of the infecting organism. We can try to place blame and there is some to go around. We should plan to have a better program for testing for the next infecting organism.
This is not a slam dunk. We don’t know what it is yet. I like Dr. Segal’s comments, because he always has both of his feet on the ground. That means a lot to me. (Pun intended)
Here are some thoughts on “competition between organisms:”
All micro-organisms on earth face competition. Covid-19 is no different. By itself, it has a very “modest” immune system, if you want to call it that. It’s cell wall in very modest by comparison to organisms that are more complex.
The problem with most estimates of the severity of the outbreak is that these “estimates” are based upon a mathematical model that assumes NO competition against the organism.
Identifying and quantifying that competition is difficult, especially at early stages. That is why those factors are not typically identified in early studies. “It is easier to present a doomsday study to Media. They will always enjoy that.” But it is less than useless, except to create hysteria. If it has any use, it is to galvanize necessary planning.
Based upon the notion of “no competition,” it is possible for any micro-organism to take over the earth. Nature has made this impossible.
Here are a list of factors that mitigate against unlimited expansion:
Exponential growth for organisms requires specific attributes:
1. Lack of competition against the infecting organism
2. Availability of energy (food) for the infecting organism
3. Adequate supply of fomites for the infecting organism
4. Lack of chance evolutionary changes that damage the infecting organism
5. Defeat of natural tendencies for (victim) organism to engage in strategies that are unknown or unexpected.
6. So-called “promiscuous opportunities” for new substrates. (This was present for AID’s)
7. Temperatures and water content must be available within the homeostatic attributes of the infecting organism. (Most organisms, including Covid-19 cannot tolerate high temperatures or ultra-violet light from direct sun exposure)
8. Lack of Artificial competition and destructive biological attacks on the infecting organism (vaccines and chemicals that do not occur in nature)
9. Availability of (unexpected) additional substrates
10. All epidemic organisms tend to follow their own virulence index. Virulence is never permanent. It always ends.
One cannot just assign a mathematical model for exponential growths and expect it to apply to Covid-19. It looks “good” on a moving mathematical computer program. But it is not reality.
There is now an “argument” over Chloroquine. The French study says it works. We will see. But even if it does, there is not enough available at the present time. It is important to PLAN for the possibility that it will work, which means manufacturing millions of new doses.
Thanks to all those in medicine and research fighting for us!! Our gratitude is as deep as the ocean.
Michael M. Rosenblatt, DPM
” We got caught with our pants down.”
How so?
We have a novel virus on our hands. China delayed in alerting us to the virus for weeks. The US Congress was hell bent on impeaching the president with the virus stories first got going. No leader or any business or organization is going to focus on outside threats when under direct legal assault. That clearly diverted attention away from the virus in the early stages.
Nevertheless, the president managed to be paying attention and stopped planes flying from China to here on January 31, 2020. At the time he was called a xenophobe and a racist, but instead he should have been called prescient.
Once the virus was identified then a test had to be developed. To ramp up to full testing capability in a period of perhaps 6-7 weeks in order to produce millions of test kits, is extraordinary.
How many test kits do we keep on the shelf for flu across the US. In this case because of media frenzy we are going to wind up testing tens of millions of people and perhaps hundreds of millions of people because of FEAR. 99% of patients are going to recover from this virus just fine. 1% or less will die. The majority will be elderly.
The all cause mortality rate for all diseases in the elderly is significant. This virus will likely be a small proportion of the all cause mortality in the elderly.
For that we have tanked our economy and our stock market. In a month when the vast majority of patients recover with no sequela, are they not going to be angry that we tanked the economy VOLUNTARILY, and shut down an entire nation. This was all done to slow the spread and decrease the burden on the “health care system”. However, was that really worth crashing the economy. How many people will be out of work and financially destroyed? How many businesses will never reopen. All of that for an at risk population that would likely have died of some other cause.
We will not know for a few more weeks about this, but we have paid a terrible price for combating this virus with a vast overreaction. In 1984 when AIDS first showed up it had a 100% mortality and we did not see hysterical panic and mass media insanity reporting every single death breathlessly.
This is all new ground for us as a country. But this virus from an economic viewpoint is going to have a greater impact than 9/11 and 2008’s crash combined. Hotels have gone from 67% occupancy to less than 10% occupancy. We are killing off many industries that will take years to recover, if ever. We will see if the price we have paid is worth the price of the lives that would likely have been lost from some other cause anyway.
Here’s how we got caught with our pants down. In hospitals across the country – but in particular in the hot spots like Washington, NY, and Bay Area, they are running out of masks, gowns, and gloves. These are products that will predictably be used. It is certain they will be used in pandemics and regular times. And they are indispensable in a pandemic where we hope to protect our front line doctors and staff. Any doctors who test positive or become sick are taken out of commission for a period of time. Why do these healthcare behemoths not have a minimum 3 month supply at ALL times. Use the oldest ones, then replace with new ones. You’d always have a 3 month supply. Same for our pharmaceuticals. In our just in time mindset, the healthcare bean counters never believed we’d have a serious problem with restocking supplies.
“Crimson Contagion” report was presented to the administration in October 2019. Its recommendations for the procedures at start of a pandemic were not followed in 2020.
Dear retired: Glad you are not actively practicing medicine because your understanding of the issue is appalling and you do not deserve the title of healer. Obviously you have made a learned decision that the death of 1% of our population is worth paying to sustain an economic system. Some of us disagree and i wonder if you will still have that same opinion when the 1% is someone you care about, if you are capable of caring.
On Retired vs. Dr Barnett
Retired says we “over-reacted” and subjected ourselves to horrendous, long-term economic damage because we wanted to “protect our elderly” , when in many cases, they would be first to die anyway.
Dr. Barnett does not appreciate that attitude and believes that we must protect our elderly at all costs.
I think you both have misplaced anger. The ANGER should go against the Chinese Communists, who have deliberately neglected to protect their own people and allowed EARLY transmission of the virus across many borders.
We all like to travel. I do too. But when you KNOW that there is an epidemic in your country, you owe it to the rest of the world to inform them early on.
The biggest argument now is: “How dangerous is globalism?” I can write a 30 page paper on this, but this is a medical site. I will simply say that (excessive) economic globalism is DANGEROUS and so is TRAVEL. Open borders are simply a “representation” of the past that is no longer tenable.
After 911, the US passed laws that allowed victims of 911 to sue Saudi Arabia. That can be done with China now.
I am 77 years old, so I am in the range of greatest risk. I am staying home. So is my wife. Thank God I no longer have to work, but some family members need my “help” which I am providing.
Retired is correct about the horrendous financial disaster this is. BUT I STILL HAVE FAITH IN AMERICA UNDER A PRESIDENT WHO IS A CAPITALIST. Ultimately I believe this will get fixed. I had to sell magazine subscriptions door to door in Detroit when I was a teen, in order to pay for my clothing and piano lessons. I understand poverty with a deep sense of personal experience.
I am not as pessimistic as retired. Perhaps I am deluded. Time will tell. But I still believe in America.
Michael M. Rosenblatt, DPM
i have no anger toward Retired. It is an opinion. i also cannot summon anger against the chinese when our own nation with nearly two months to prepare chose to dawdle. My father who was a child during the Great Depression when they did not go to the doctor because it cost money, when they could not afford shoes and made clothes out of flour sacks remembers that time of his life as one of the happiest times of his life. They had family, their single mom of five managed to keep some food usually cornbread and some bacon grease on the table and they huddled together to listen to the radio at night to conserve heat. Health and relationships are EVERYTHING. i am deeply passionate about that and have little time for anger as i am trying to make sure that my patients who are scared shitless understand we are still here for them, cancelling and refunding all my elective surgeries for an unforeseeable future, shopping for my quarantine supplies and deciding how to provide for my employees, most of whom are single moms. i made the sad decision to terminate my highest paid employee, the PA because i can keep the others on for quite some time with her salary. She is pregnant and they are inducing her next week so she does not deliver in the middle of a pandemic. And do not be mistaken, the elderly while disproportionately affected by this virus will not be alone. My colleagues in Seattle tell us they lost an 18 yo and 20 yo on Monday who had no comorbidities so please, go ahead and roll the dice with your loved ones for the sake of $s! i am proud to sign my name to this!
In no way can any physician turn their back on patients. Yet, this happens in triage. I have always been uncomfortable with that concept. Turning to triage in an otherwise rich country is obscene.
There is blame to go around. But I am not quite so willing to give China a “free ride” on this, even if we “dawdled.” We have to recognize that there are some aspects of cultures, including our own, that are not always positive and helpful. Some cause enormous damage.
I can suggest for example, that our movie and entertainment industry have “pushed” recreational drug use, rampant promiscuity, violence for the sake of violence and a mantra that suggests the “world is meaningless and there is no over-riding morality.” (Coen Brother’s movies.)
Turning to the Chinese, there seems to be a proclivity to “saving face” that in this case has directly resulted in a pandemic. This combined with a Communist Party that fears anything negative about itself, furthered an unnecessary spread. There has always been a tendency for Asian people to eat anything. In the distant past of starvation, perhaps this was understandable.
But in modern times it has turned into a kind of “cultural pica.” Acres of half living, dehydrated creatures, slaughtered on site is not healthy or normal. It is not racist to point this out. Yet, this has been going on for years. I saw it myself. It was disgusting and horrible.
Sorry, I do not excuse the Chinese for this. I don’t excuse the Coen Brothers either for their awful message and refuse to see their movies. We can “blame” cultures. It is not racist.
We have a right and an obligation to hold the Chinese Government responsible in Court for what they put us through.
Michael M. Rosenblatt, DPM
All of us in NJ should be very careful for the next couple of weeks. We closed our office for at least 2 weeks after seeing the spike in covid19 admissions to Our local hospital from last Tuesday to Thursday. The hospitals’ ICUs in NJ are a mess and will get worse. The problem is that the asymptomatic carrier doesn’t know he’s contagious because he’s incubating virus. The mean incubation period for covid19 is 7 days, and tops of 14 days. Plus the state will stop any elective surgery this week I suspect to conserve masks and gloves that are already on backorder. This too shall pass, but strict “social distance” with family and kids is essential now. When the curve declares itself, and when the hospitals lighten, we will reopen. May God bless all of us.
There is no time or energy to be WASTED ON BLAME. I am an ER MD on the Gulf Coast and although we haven’t started our predicted rush yet I have been treating cases since March 12th. The variation in initial presentation, presence of asymptomatic carrier status, rapid decompensation, long incubation and the ferocity of the cytokine reaction are just some of the many unprecedented things we are seeing that are creating a perfect storm. If you can help in any way, maybe get involved with telemedicine efforts if you are a high risk player, then please do so. I can see no way that we will not lose providers at all levels and we are going to need all hands on deck